
Improving the precision of behaviour change theories: Development and validation of a dynamic COMPutational model of LAPSE risk in smokers attempting to stop (COMPLAPSE)
COMPLAPSE was funded between 2022-2025 by the European Commission under the Horizon Europe Framework Programme (HORIZON), Grant No. 101065293 (PI: Dr. Olga Perski; Mentors: Prof. Nelli Hankonen and Prof. Eric Hekler). This website is used for the dissemination of the project findings, including links to scientific publications, presentations and videos.
Brief project summary
The EU-funded project, COMPLAPSE, developed a formal and computational model of smoking lapse and relapse. We combined scientific theory, patient perspectives, and clinical know-how. The model, available as an interactive web app, can be used to simulate relapse risk and inform personalised, evidence-based digital cessation strategies.
Discover how COMPLAPSE is turning complexity into actionable insights for public health.
Watch the video (produced by Booster):
Aims and objectives
Cigarette smoking remains the leading preventable cause of premature morbidity and mortality in Europe and beyond. Gold standard treatment for smoking cessation includes pharmacotherapy and behavioural support. However, smoking lapses – influenced by momentary fluctuations in cigarette availability, stress, and cravings – are a key source of treatment failure. COMPLAPSE aims to advance the state-of-the-art by developing and validating a formal, dynamical systems model of lapse risk, improving the precision of static behaviour change theories to account for observed complexities and laying the foundation for dynamically tailored, person-centred digital smoking cessation interventions for increased effectiveness. COMPLAPSE is interdisciplinary in scope – drawing on know-how from behavioural science, systems science and dynamical systems modelling – and directly contributes to Europe’s Path to the Digital Decade and its Strategic Framework for the Prevention of Non-Communicable Diseases. COMPLAPSE aims to address the following Research and Innovation Objectives (ROIs), with each ROI associated with a dedicated Work Package (WP):
ROI1. To develop a conceptual model of lapse risk, drawing on stakeholder input and the researcher’s knowledge of the available literature via participatory systems mapping (WP1).
ROI2. To formulate mathematical equations for each component in the conceptual model and conduct a series of computer simulations (WP2).
ROI3. To collect and analyse EMA and sensor data and use this to validate the expert-derived dynamic computational model (WP3).
WP1
Theories are needed to predict, explain, and influence phenomena of interest. Popular relapse prevention theories are vaguely specified using natural language descriptions and lack temporal information about how key phenomena (i.e., ‘relapse’, ‘prolapse’, ‘abstinence’) are dynamically caused over time and within individuals. Formal modelling involves the translation of a theory’s structure into a mathematical framework and can help mitigate the ongoing ‘theory crisis’ in psychology and related disciplines, which contributes to the wider reproducibility crisis.
The aim of WP1 was to develop a conceptual model of lapse risk in smokers attempting to stop, with a view to using this to formulate a formal and computational model. However, due to the lack of fit-for-purpose methodological guidance, we first conducted a scoping review to examine the extent and nature of research activities pertaining to the use of formal and computational modelling to predict, explain and influence health behaviours unfolding at the within-person level. We synthesised methodological steps in the published literature and generated a set of initial, expert-derived ‘best practice’ modelling recommendations.
In addition, since formal and computational modelling has been used for decades in other scientific disciplines, we also took a broader perspective and conducted another scoping review in which we synthesised modelling guidance from diverse disciplines (e.g., psychology, engineering, biology, physics). The two scoping reviews (and the ongoing discussions with the involved interdisciplinary researchers) informed the next steps of our research.
After conducting the scoping reviews, we drew on the Theory Construction Methodology to develop a dynamic model of smoking lapse and relapse. We used a participatory, multi-method approach to iteratively develop the conceptual model (also referred to as a ‘prototheory’), which included: i) an informal theory review of popular lapse and relapse theories; and ii) two linked stakeholder interviews with researchers, people with lived experience, stop smoking practitioners, and policymakers (N = 15).
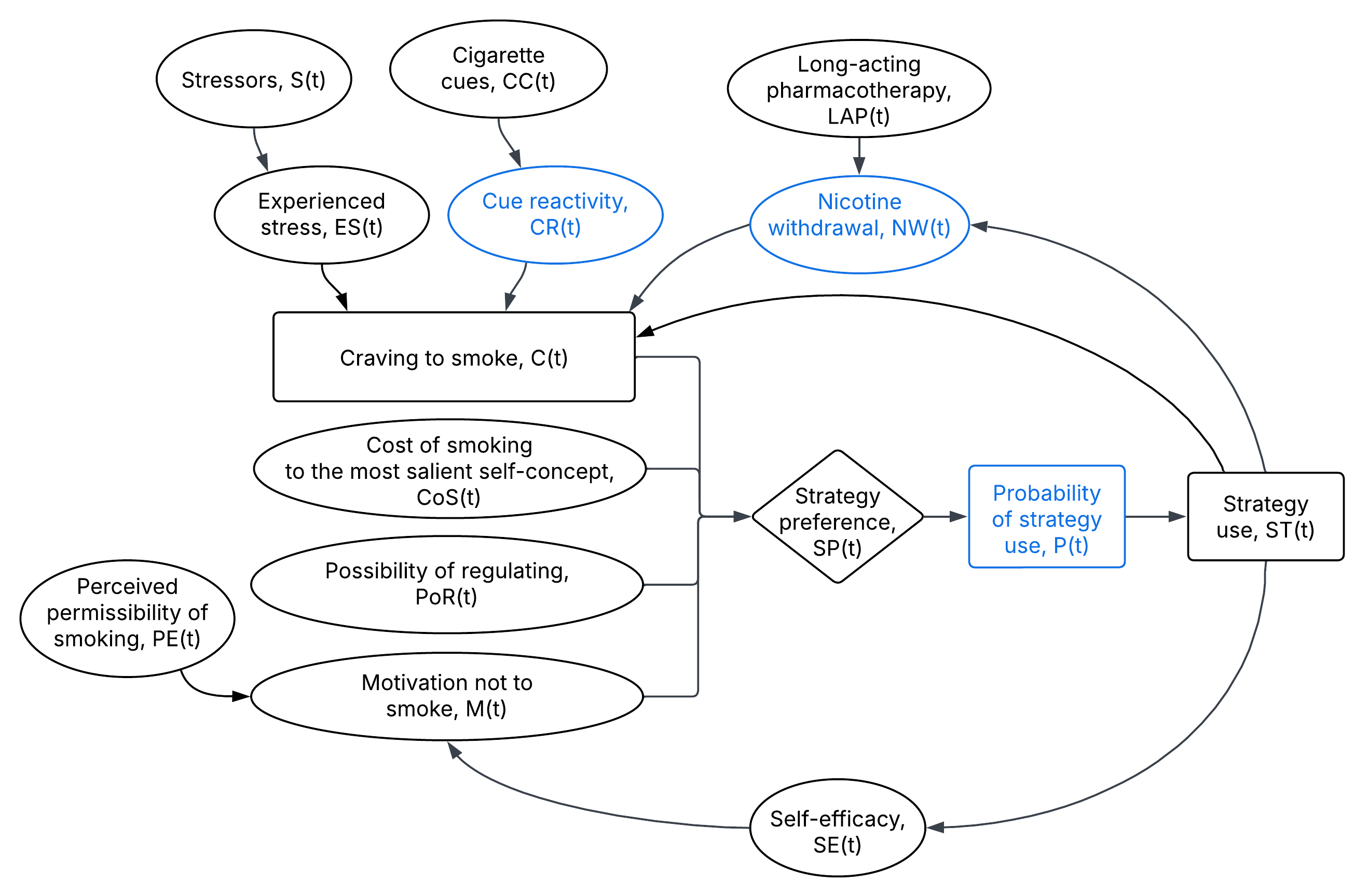
WP2
Next, we translated the prototheory into a series of difference equations which were implemented in R code and an R Shiny application, which enables interested users to explore the dynamic model on their own. We conducted a series of computer simulations to examine if the formal and computational model could produce the empirical phenomena which it set out to explain (i.e., ‘relapse’, ‘prolapse’, ‘abstinence’). The stakeholders were invited back to provide feedback on the simulated model outputs. Their feedback was incorporated into an updated model version. A paper describing the development and initial evaluation of the formal and computational model of lapse risk has been submitted for publication and is available as a pre-print.
We also wrote a magazine article to describe how we worked together - integrating know-how from health psychology and mathematics/modelling - to translate the prototheory into a formal and computational model:
WP3
In the final stage of project COMPLAPSE, we are collecting EMA and smartwatch data to empirically evaluate the dynamic model of lapse and relapse. Data collection is still ongoing. We will fit the formal model to the data from each participant and calculate goodness-of-fit statistics.